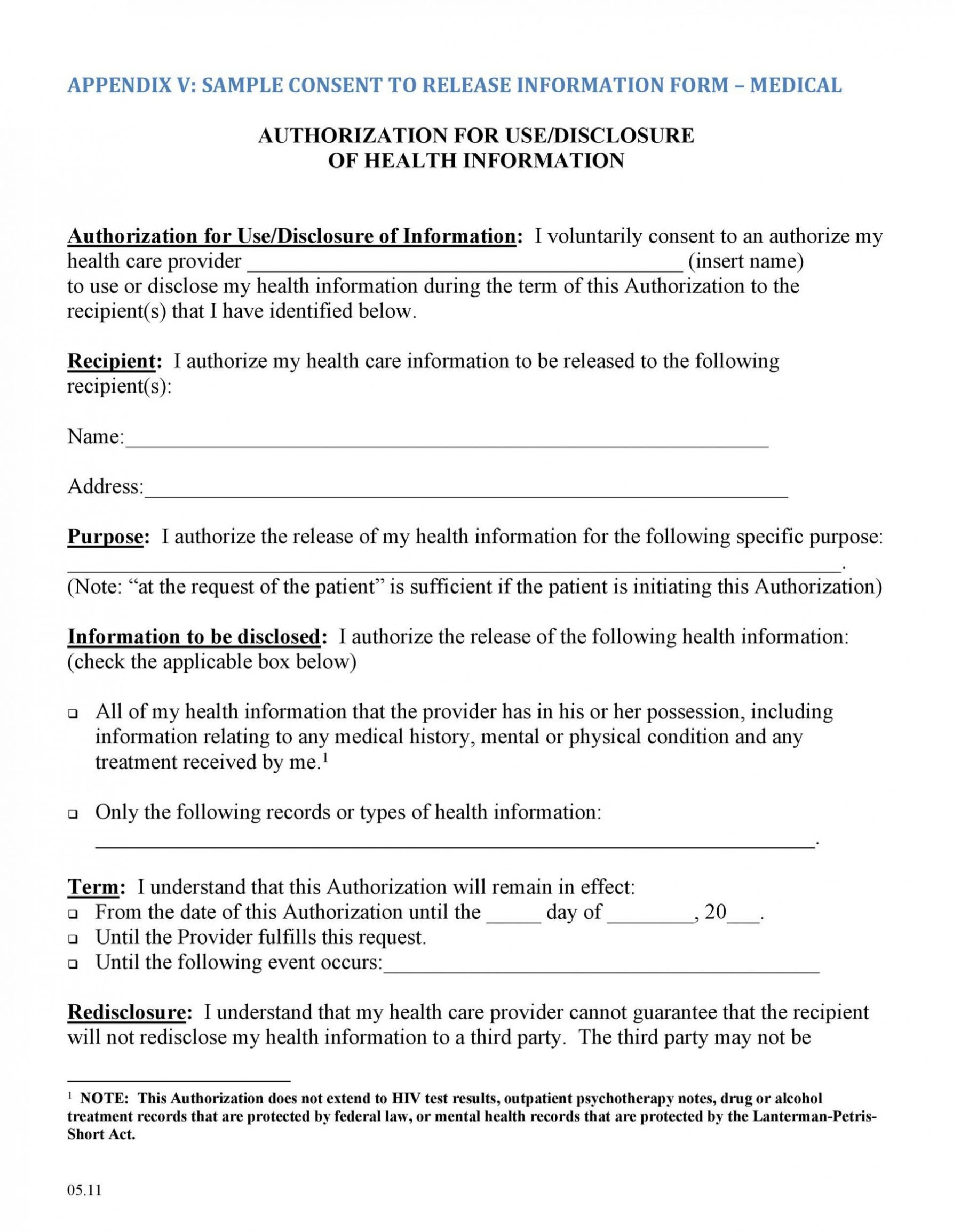
Release Of Information Form Mental Health Template - I understand that i have the right to revoke this authorization at any. A mental health release of information form allows mental health practitioners to legally disclose a patient's confidential. Sample standard authorization mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert. Full treatment record including all health/mental. This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. To release, discuss, or disclose the following: This authorization will expire on (date): Full treatment record excluding the following information: This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. I, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form in.
This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. Sample standard authorization mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert. I understand that i have the right to revoke this authorization at any. This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. I, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form in. A mental health release of information form allows mental health practitioners to legally disclose a patient's confidential. Full treatment record including all health/mental. Full treatment record excluding the following information: To release, discuss, or disclose the following: This authorization will expire on (date):
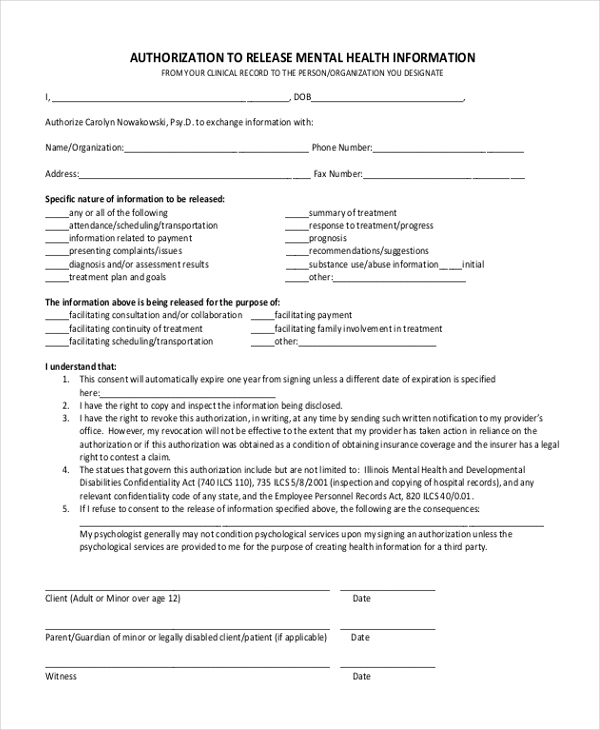
Sample standard authorization mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert. This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. This authorization will expire on (date): I understand that i have the right to revoke this authorization at any. I, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form in. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. To release, discuss, or disclose the following: Full treatment record excluding the following information: A mental health release of information form allows mental health practitioners to legally disclose a patient's confidential. Full treatment record including all health/mental.
Free Mental Health Release Of Information Form
Full treatment record including all health/mental. I, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form in. To release, discuss, or disclose the following: A mental health release of information form allows mental health practitioners to legally disclose a patient's confidential. This template can be used to coordinate.

Release of Information Form Four County Mental HEvalth Center Fill
A mental health release of information form allows mental health practitioners to legally disclose a patient's confidential. This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. I, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form in. This template.

Release of information template Fill out & sign online DocHub
This authorization will expire on (date): Sample standard authorization mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert. Full treatment record including all health/mental. I understand that i have the right to revoke this authorization at any. A mental health release of information form allows mental health practitioners to legally disclose a patient's.
Sample Release Of Information Form Mental Health Classles Democracy
I understand that i have the right to revoke this authorization at any. This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. I, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form in. A mental health release of information.
Sample Release Of Information Template Addictionary Mental Health
Full treatment record excluding the following information: Sample standard authorization mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert. I, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form in. A mental health release of information form allows mental health practitioners.

Mental Health Release Of Information Form & Template Free PDF Download
Sample standard authorization mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert. Full treatment record including all health/mental. A mental health release of information form allows mental health practitioners to legally disclose a patient's confidential. I understand that i have the right to revoke this authorization at any. This form provides your therapist.
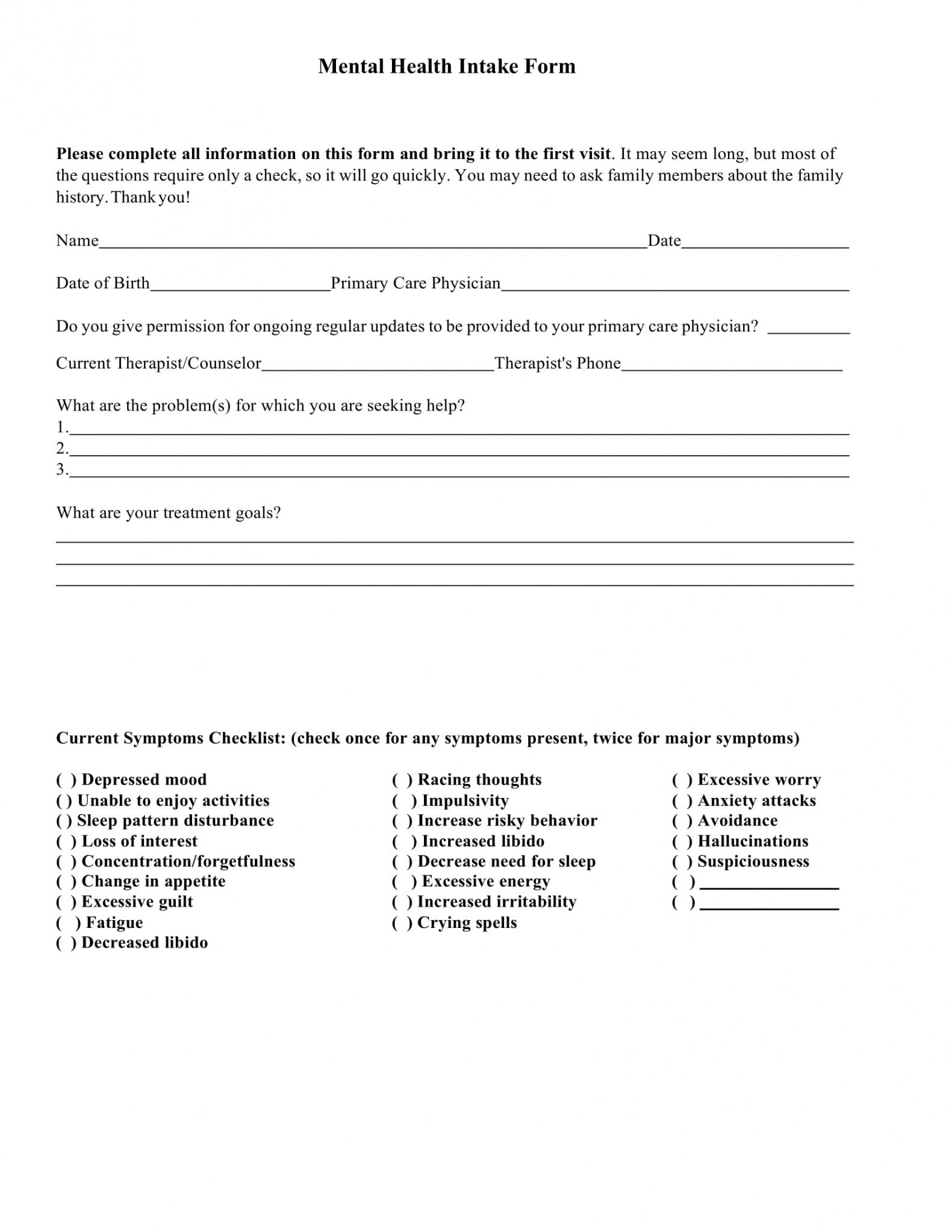
Free 9 Mental Health Providers Intake Forms In Pdf Ms Word Mental
Full treatment record excluding the following information: I understand that i have the right to revoke this authorization at any. This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where.
Free Release Of Information Form Mental Health Template Doc
Full treatment record including all health/mental. I, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form in. I understand that i have the right to revoke this authorization at any. A mental health release of information form allows mental health practitioners to legally disclose a patient's confidential. Sample.

FREE 9+ Sample Release of Information Forms in MS Word PDF
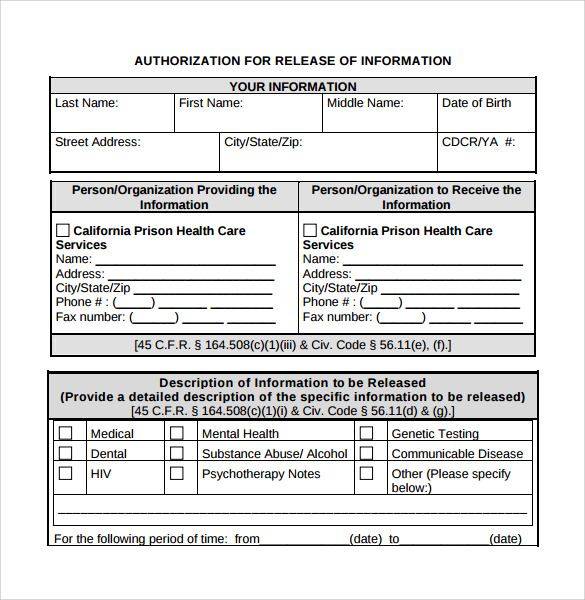
This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. I, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form in. To release, discuss, or disclose the following: This template can be used to coordinate the release of confidential information.

Free Sample Counseling Release Of Information Form
This authorization will expire on (date): I understand that i have the right to revoke this authorization at any. A mental health release of information form allows mental health practitioners to legally disclose a patient's confidential. Sample standard authorization mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert. I, or my authorized representative,.
I, Or My Authorized Representative, Request That Health Information Regarding My Care And Treatment Be Released As Set Forth On This Form In.
A mental health release of information form allows mental health practitioners to legally disclose a patient's confidential. Full treatment record excluding the following information: I understand that i have the right to revoke this authorization at any. Sample standard authorization mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert.
This Form Provides Your Therapist With Written Permission To Communicate With Other Individual Providers Regarding Your Treatment (E.g.
This authorization will expire on (date): This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. Full treatment record including all health/mental. To release, discuss, or disclose the following: