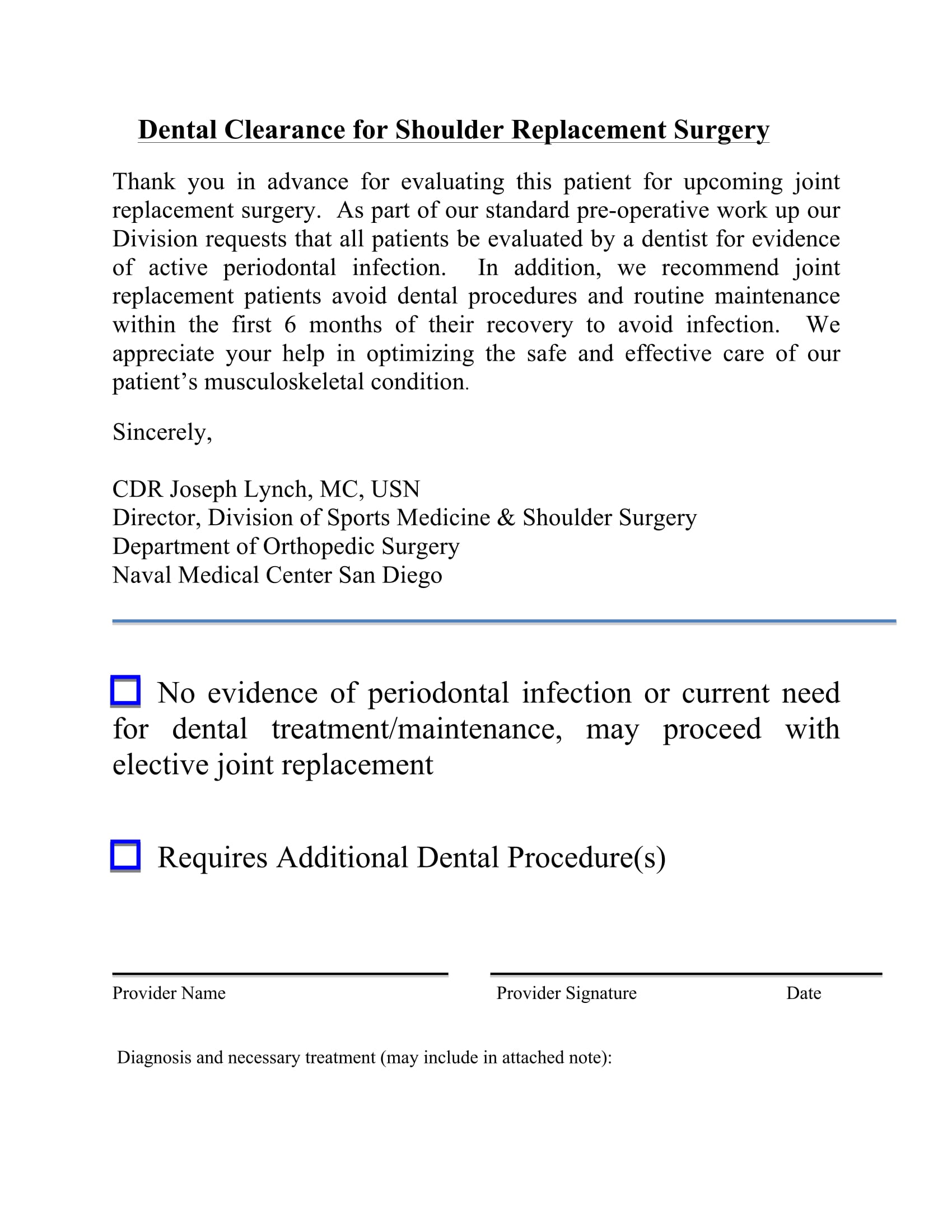
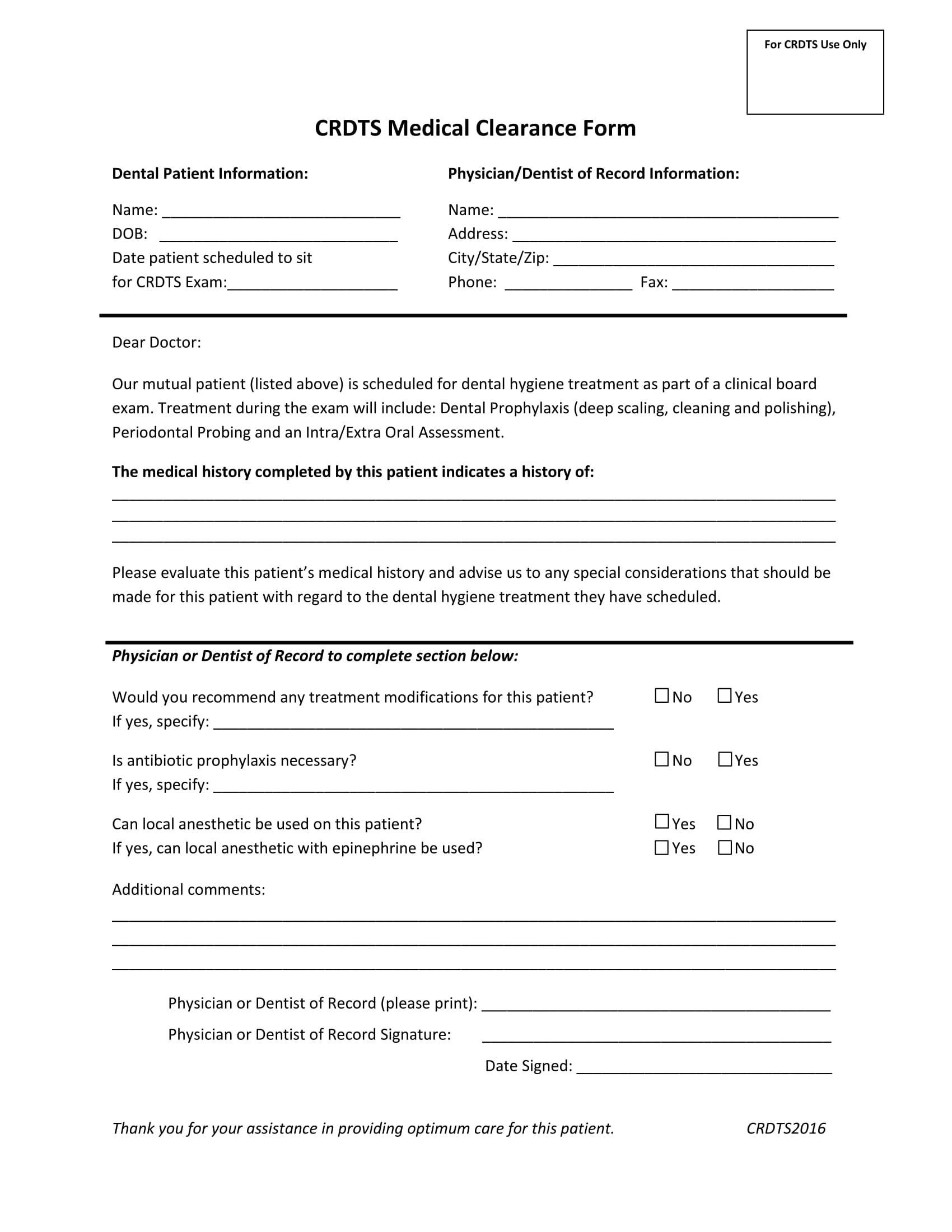
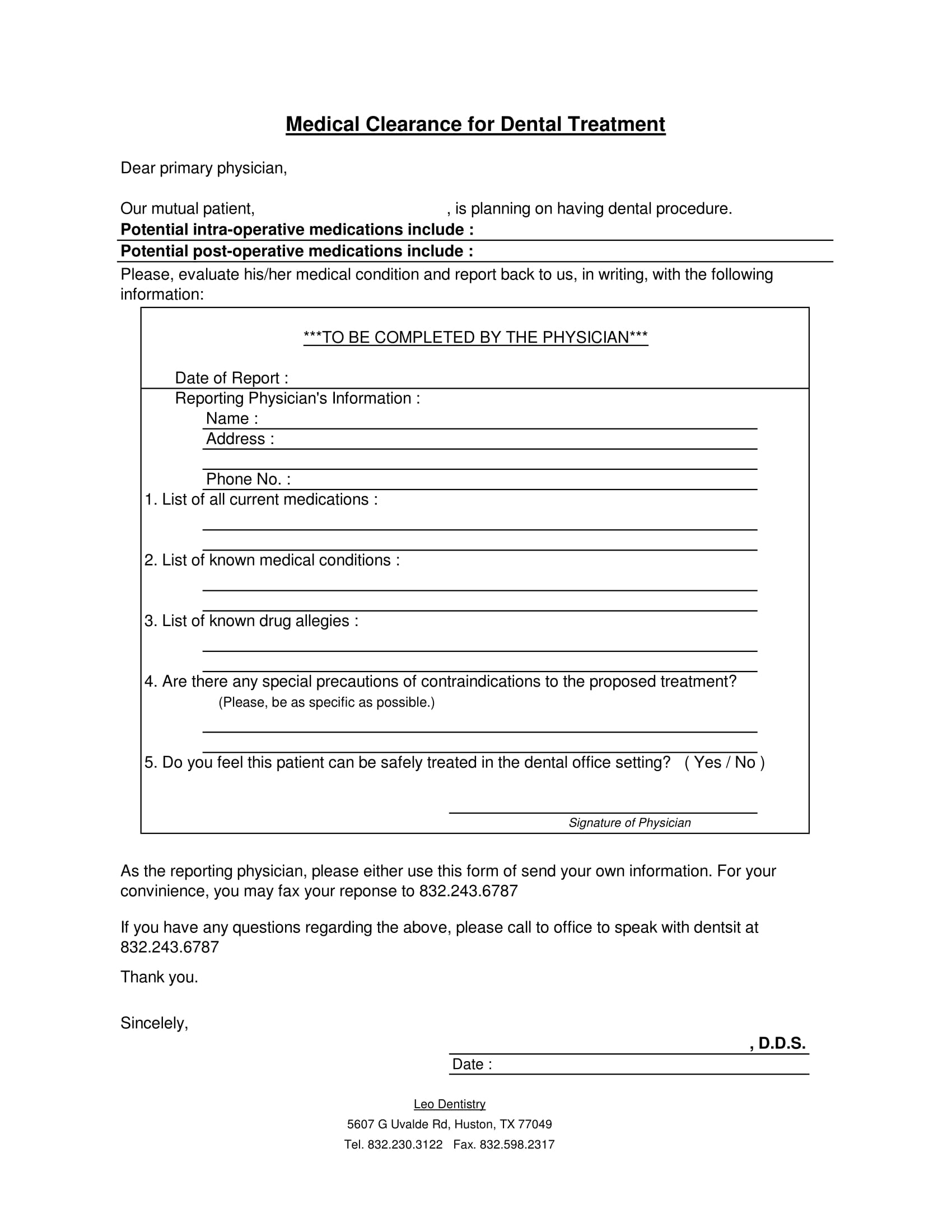
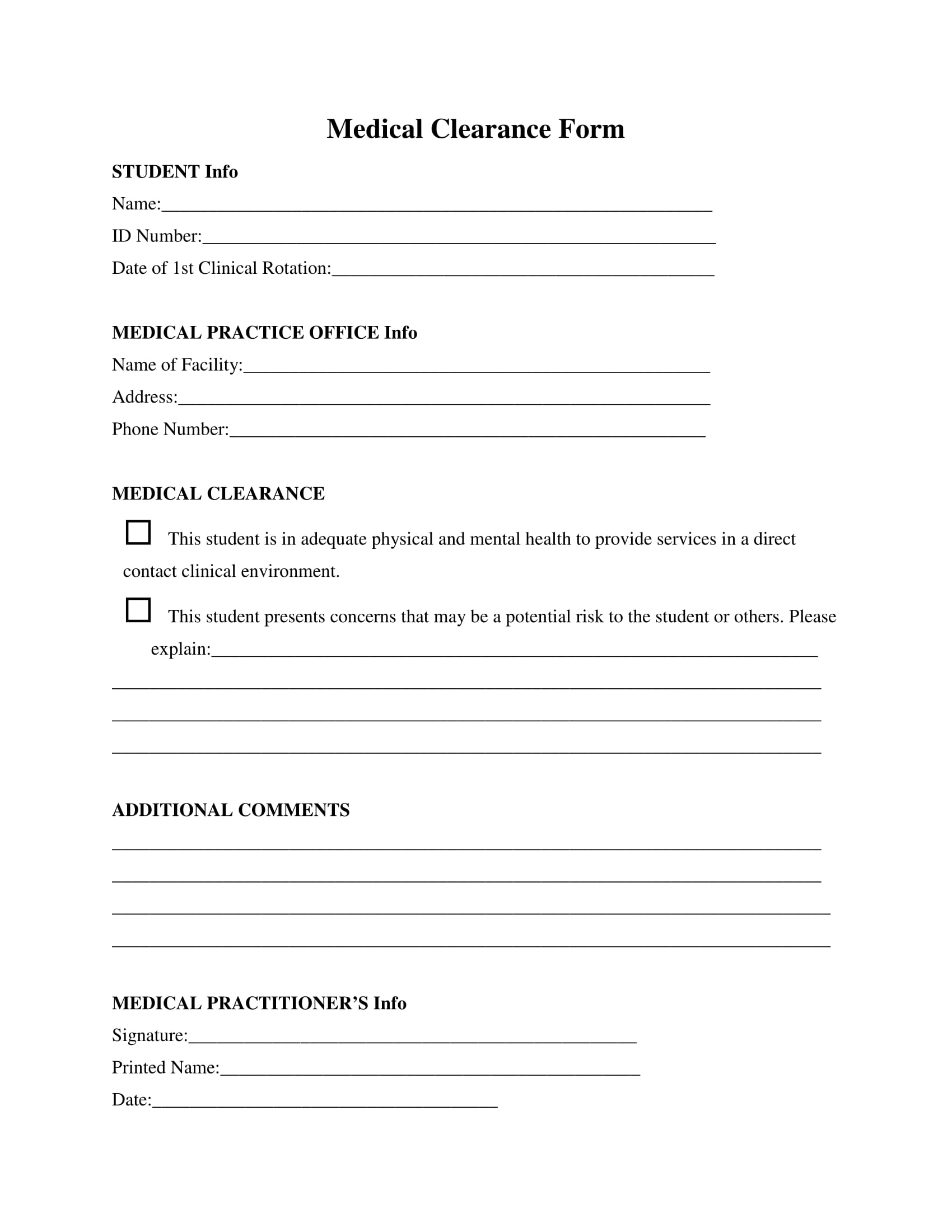
Printable Medical Clearance Form For Dental Treatment - Sign, print, and download this pdf at printfriendly. The patient has indicated the following medical conditions: Dentist name (please print) patient signature date physicians: Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical. It ensures that the patient's medical history is reviewed by a. View the medical clearance for dental treatment form in our collection of pdfs. This form is essential for obtaining medical clearance prior to dental treatment.
This form is essential for obtaining medical clearance prior to dental treatment. View the medical clearance for dental treatment form in our collection of pdfs. The patient has indicated the following medical conditions: Sign, print, and download this pdf at printfriendly. Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical. It ensures that the patient's medical history is reviewed by a. Dentist name (please print) patient signature date physicians:
It ensures that the patient's medical history is reviewed by a. Dentist name (please print) patient signature date physicians: The patient has indicated the following medical conditions: This form is essential for obtaining medical clearance prior to dental treatment. Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical. Sign, print, and download this pdf at printfriendly. View the medical clearance for dental treatment form in our collection of pdfs.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
View the medical clearance for dental treatment form in our collection of pdfs. This form is essential for obtaining medical clearance prior to dental treatment. Dentist name (please print) patient signature date physicians: Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical. It ensures that the patient's medical history is reviewed by a.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
View the medical clearance for dental treatment form in our collection of pdfs. Sign, print, and download this pdf at printfriendly. Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical. It ensures that the patient's medical history is reviewed by a. The patient has indicated the following medical conditions:
FREE 30+ Medical Clearance Forms in PDF MS Word
Sign, print, and download this pdf at printfriendly. Dentist name (please print) patient signature date physicians: This form is essential for obtaining medical clearance prior to dental treatment. View the medical clearance for dental treatment form in our collection of pdfs. The patient has indicated the following medical conditions:
FREE 30+ Medical Clearance Form Samples in PDF MS Word
View the medical clearance for dental treatment form in our collection of pdfs. The patient has indicated the following medical conditions: It ensures that the patient's medical history is reviewed by a. Dentist name (please print) patient signature date physicians: Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical. Sign, print, and download this pdf at printfriendly. View the medical clearance for dental treatment form in our collection of pdfs. The patient has indicated the following medical conditions: This form is essential for obtaining medical clearance prior to dental treatment.
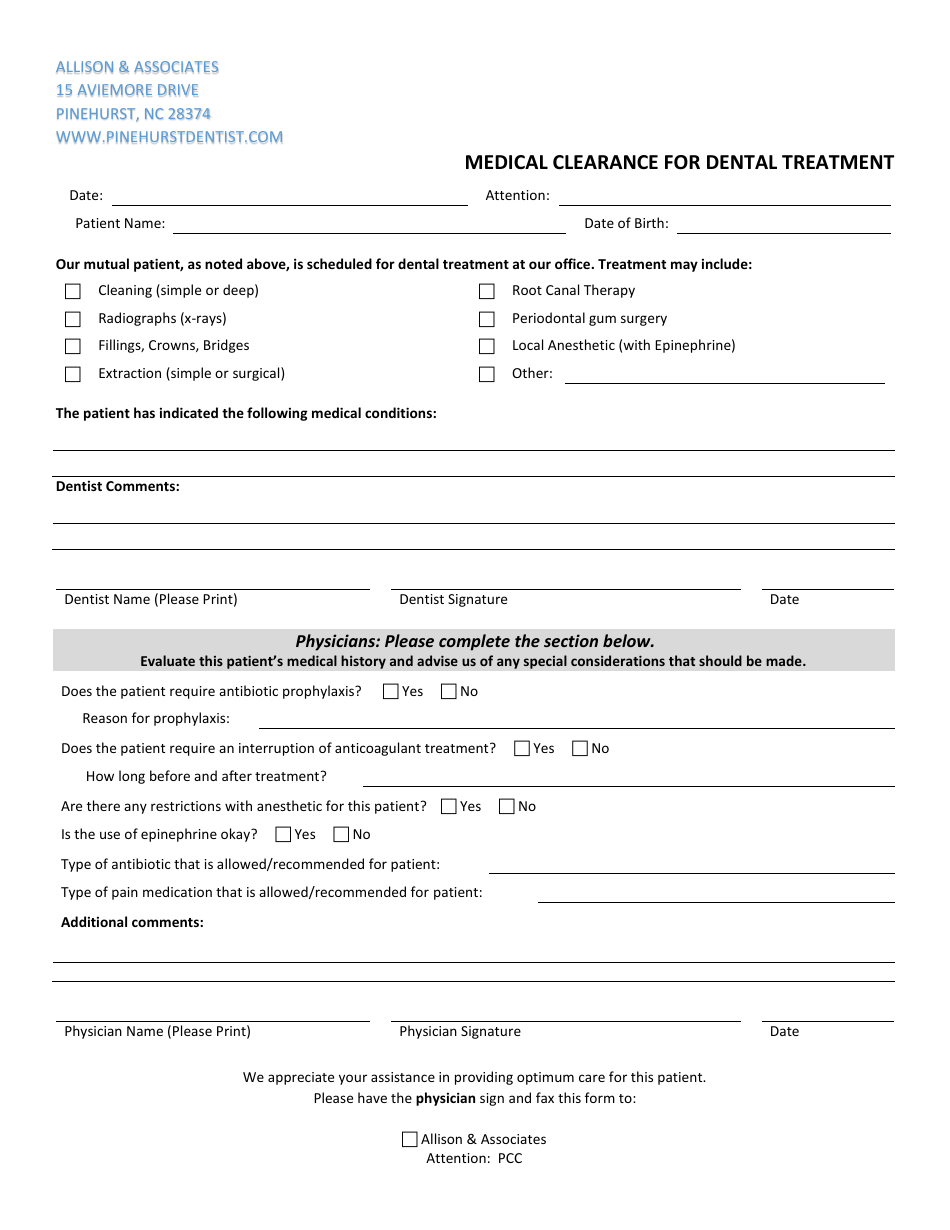
Medical Clearance for Dental Treatment Allison & Associates Download
It ensures that the patient's medical history is reviewed by a. Dentist name (please print) patient signature date physicians: Sign, print, and download this pdf at printfriendly. The patient has indicated the following medical conditions: Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
It ensures that the patient's medical history is reviewed by a. Sign, print, and download this pdf at printfriendly. The patient has indicated the following medical conditions: View the medical clearance for dental treatment form in our collection of pdfs. Dentist name (please print) patient signature date physicians:
Printable Medical Clearance Form For Dental Treatment
This form is essential for obtaining medical clearance prior to dental treatment. It ensures that the patient's medical history is reviewed by a. Sign, print, and download this pdf at printfriendly. The patient has indicated the following medical conditions: View the medical clearance for dental treatment form in our collection of pdfs.
FREE 30+ Medical Clearance Form Samples in PDF MS Word
View the medical clearance for dental treatment form in our collection of pdfs. It ensures that the patient's medical history is reviewed by a. Dentist name (please print) patient signature date physicians: Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical. This form is essential for obtaining medical clearance prior to dental treatment.

Printable Medical Clearance Form For Dental Treatment
View the medical clearance for dental treatment form in our collection of pdfs. This form is essential for obtaining medical clearance prior to dental treatment. It ensures that the patient's medical history is reviewed by a. Dentist name (please print) patient signature date physicians: Sign, print, and download this pdf at printfriendly.
The Patient Has Indicated The Following Medical Conditions:
This form is essential for obtaining medical clearance prior to dental treatment. Dentist name (please print) patient signature date physicians: View the medical clearance for dental treatment form in our collection of pdfs. It ensures that the patient's medical history is reviewed by a.
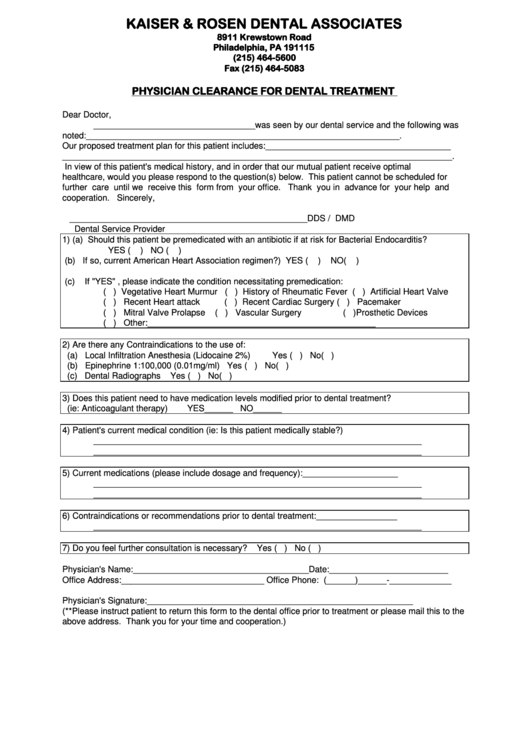
Medical Clearance For Dental Treatment Patient’s Name:_________________________ D.o.b:______________ Date Of Last Physical.
Sign, print, and download this pdf at printfriendly.