New Patient Medical History Form Template - New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if. Please complete this form to provide information regarding your medical condition. Feel free to ask your primary care physician for assistance.
Please complete this form to provide information regarding your medical condition. Feel free to ask your primary care physician for assistance. New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if.
Feel free to ask your primary care physician for assistance. Please complete this form to provide information regarding your medical condition. New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if.
Comprehensive Health History Template
Feel free to ask your primary care physician for assistance. Please complete this form to provide information regarding your medical condition. New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if.
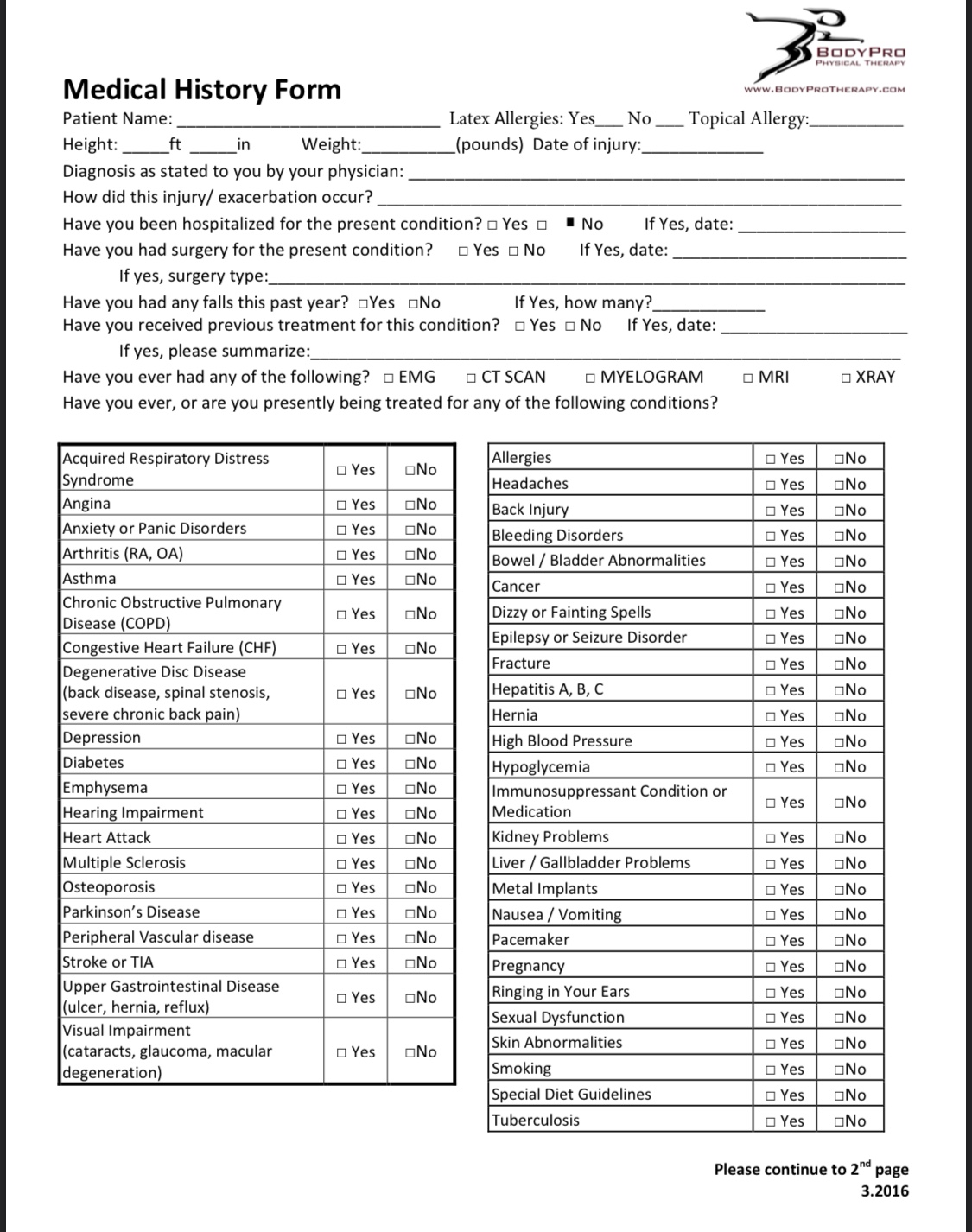
![43 Formularios de historial de salud médica [PDF, Word] Mundo Plantillas](https://mundoplantillas.com/wp-content/uploads/2022/06/health-history-form-33-scaled-1-791x1024.jpg)
43 Formularios de historial de salud médica [PDF, Word] Mundo Plantillas
Feel free to ask your primary care physician for assistance. New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if. Please complete this form to provide information regarding your medical condition.

New Patient Health History Form Template 20202022 Fill and Sign
New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if. Feel free to ask your primary care physician for assistance. Please complete this form to provide information regarding your medical condition.
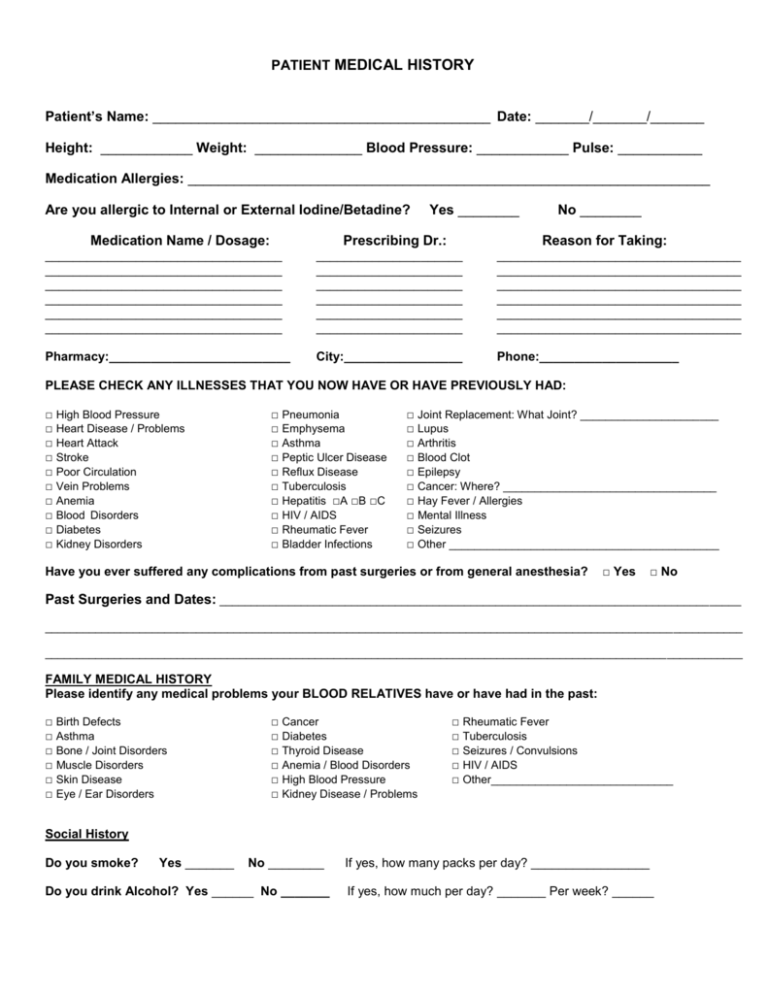
![43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2021/02/health-history-form-30.jpg)
43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab
Feel free to ask your primary care physician for assistance. New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if. Please complete this form to provide information regarding your medical condition.
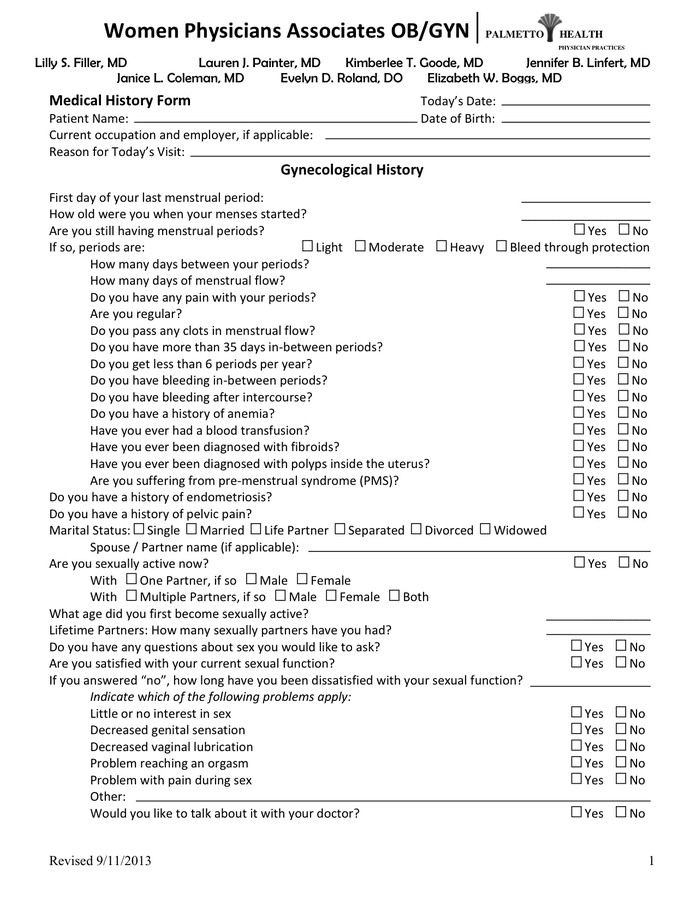
![43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2021/02/health-history-form-13.jpg)
43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab
Please complete this form to provide information regarding your medical condition. New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if. Feel free to ask your primary care physician for assistance.
New Patient Medical History Form Printable
Feel free to ask your primary care physician for assistance. Please complete this form to provide information regarding your medical condition. New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if.
New Patient Medical History Form in Word and Pdf formats
Please complete this form to provide information regarding your medical condition. Feel free to ask your primary care physician for assistance. New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if.
FREE 12+ Sample Medical History Forms in PDF MS Word Excel
New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if. Please complete this form to provide information regarding your medical condition. Feel free to ask your primary care physician for assistance.
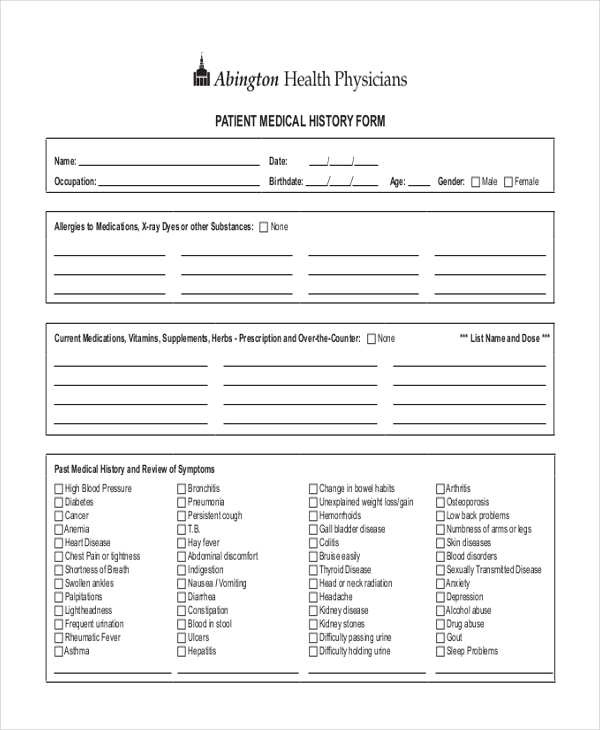
![43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2021/02/health-history-form-26.jpg)
43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab
Feel free to ask your primary care physician for assistance. Please complete this form to provide information regarding your medical condition. New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if.
New Patient Medical History Form Template PDF Template
Please complete this form to provide information regarding your medical condition. New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if. Feel free to ask your primary care physician for assistance.
New Patient Medical History Form Allergy Allergic Reaction Medications (Please List All) Dose Times Per Day (Mg., Pill, Etc.) If.
Please complete this form to provide information regarding your medical condition. Feel free to ask your primary care physician for assistance.